Gm online assessment
This is an online elog documenting de-identified patient health data after taking his signed consent to enforce a greater patient centered learning.
The privacy of the patient is being entirely conserved. No identifiers shall be revealed through out the piece of work whatsoever.
CASE DISCUSSION :
A 65 yr old female coming from Rajavaram ,was brought to the casualty with
CHIEF COMPLAINTS of:
Difficulty in moving left upper limbs and lower limbs since 3 days.
Weakness in right and left upper limbs and lower limbs since 3 days
Inability to speak since 3 days.
HOPI
Patient was apparently asymptomatic 3 days back she developed weakness in Saturday in left upper and lower limbs which was sudden in onset , gradually progressed and is completely unable to move since 3 days.
She is also unable to speak due to deviation of mouth later that day
Next day ,the weakness of both limbs of left side became severe and completely lost her speech and not responding to commands.
She lost her consciousness and urinated involuntary and left sided hemiplagia occured and lost her speech and was bed ridden for 2 days.
No H/O Head Trauma (for haemorrhagic stroke)
No H/O Epilepsy
No H/O projectile vomiting, headache or blurring of vision
No H/O recent surgeries (for embolic stroke)
PAST HISTORY:
No H/O similar complaints in the past
She is a known case of hypertension and is on medication since 2 years.
-No H/O DM, TB, Hypo/Hyperthyroidism/ Epilepsy/ Asthma/COPD/ CAD/ Blood transfusions/ Connective tissue disorders (stroke in young)
-No H/O Major hospitalizations
-No H/O major surgeries.
PERSONAL HISTORY:
➤Patient is married .
➤Patient takes mixed diet and has a decreased appetite.
➤Bowel and bladder movements are regular
➤No known allergies .
➤No addictions
FAMILY HISTORY: Not significant.
GENERAL EXAMINATION:
Patient is drowsy, non coherent and not cooperative.
Vitals:
BP: 150/80 mmHg
PR: 104 bpm
TEMPERATURE:102 degree F
RR:22cpm
Grbs 86 mg/dl
No pallor, icterus, cyanosis, clubbing,lymphadenopathy, pedal edema
SYSTEMIC EXAMINATION:
CVS‐ S1 S2 heard, no murmurs
RS‐ Normal vesicular breath sounds heard
P/A - No tenderness, no palpable mass
CNS Examination:
HIGHER MENTAL FUNCTIONS:
DROWSY, NON RESPONSIVE
GCS:E5V2M6
MMSE couldn't be assessed
speech : nil
Behavior : couldn't be assessed
Memory : couldn't be assessed
CRANIAL NERVE EXAMINATION:
3rd,4th,6th : pupillary reflexes present.
No Nystagmus
MOTOR EXAMINATION:
Right Left
UL LL UL LL
BULK: N N N N
TONE: Hyper Hyper N N
POWER: couldnt be assesssed
SUPERFICIAL REFLEXES:
Corneal present present
CONJUNCTIVAL present present
PLANTAR flexor mute
DEEP TENDON REFLEXES:
BICEPS 2+ 1+
TRICEPS 2+ 1+
SUPINATOR 2+ 1+
KNEE 2+ 1+
ANKLE 2+ 1+
SENSORY EXAMINATION:
couldn't be assessed
CEREBELLAR EXAMINATION
couldn't be assessed
SIGNS OF MENINGEAL IRRITATION: absent
GAIT couldn't be assessed
Cerebellar functions : couldn't be assessed
Provisional diagnosis:
Rt CVA with left hemiplegia with global aphasia
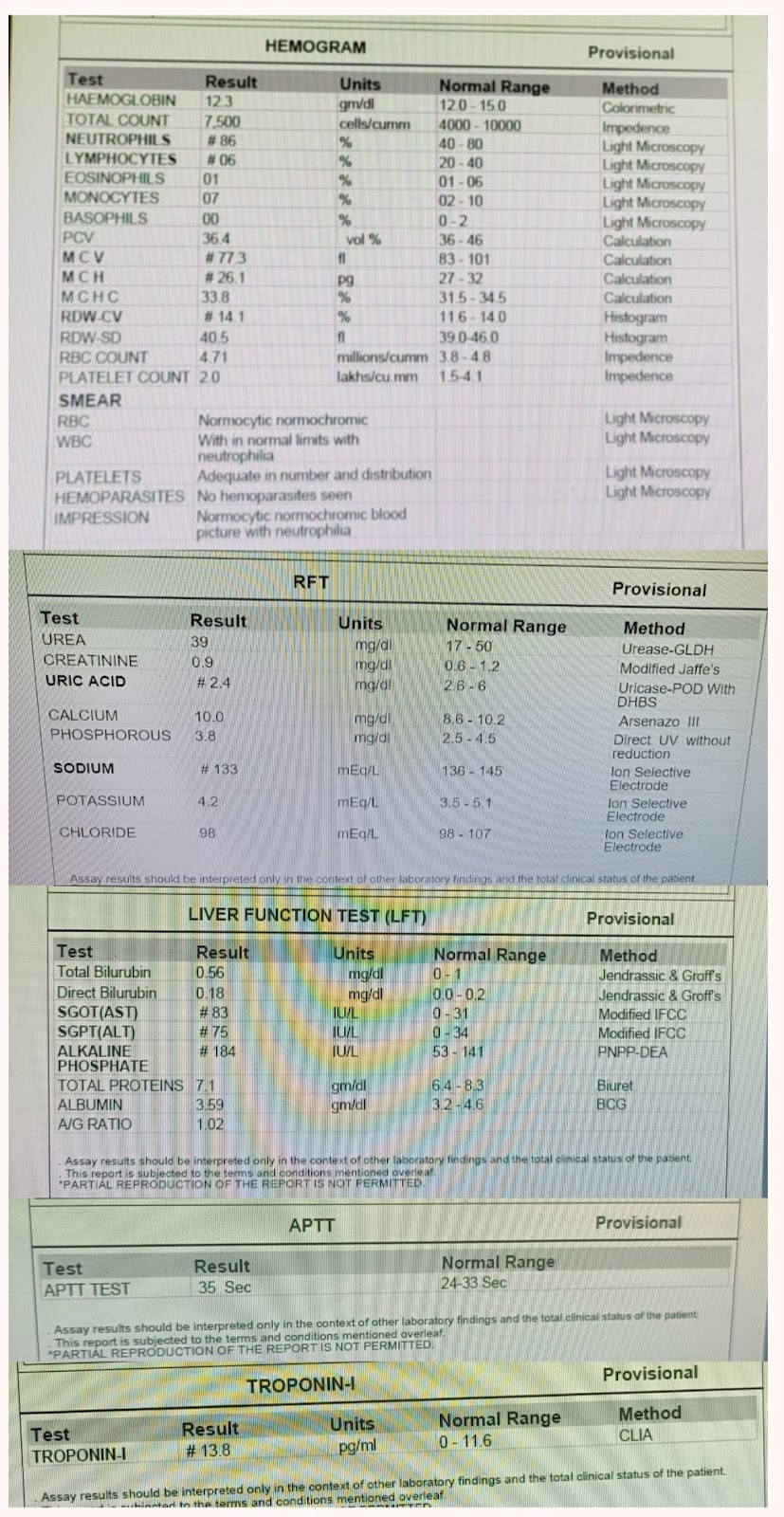
Investigations:
Chest x-ray:

DIAGNOSIS:
Right sided CerebroVascular Accident with left sided Hemiplegia with involvement of area supplied by middle cerebral artery due to embolism .
Plan of management:
1) Ryle 's tube
2) IV FLUIDS
3) Tab ECOSPRIN 150 MG RT STAT
F/B TAB ECOSPRIN 75 mg RT OD
4)Tab ROSUVASTATIN 40 MG RT STAT
F/B TAB ROSUVASTATIN 20 MG RT OD
5) TAB CLOPIDOGREL 150 Mg RT STAT
F/B TAB CLOPIDOGREL 75 mg RT OD
