Gm case 13/4/23
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
 Xray:
Xray:




I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 32yr old male patient who is a resident of miryalaguda , came with,
Chief complaints: of:
Fever since 7 days
Pain abdomen since 7 days .
History of present illness:
Patient was apparently asymptomatic 7 days back then he had fever which is sudden in onset,high grade and with chills and rigors, with body aches, and releived by taking medication. Pain abdomen since 7 days in right hypochondriac,right lumbar, umbilical region, which is needle pricking type of pain , aggrevated during expiration. Not relieved on medication .
No h/o chest pain,sob, palpitations
No h/o nausea, vomiting
No h/o loose stools
No h/o increased or decreased urine output
Past history:
Not k/c/o HTN,DM,TB, EPILEPSY,CVA
Family history:- not significant
Personal history:
Appetite:- normal
Diet:- mixed
Sleep :- adequate
B& B :- regular.
Addictions: consumes alcohol, twice a week .
(90ml) whisky
General examination:-
Patient is conscious, coherent, cooperative
Moderately built, moderately nourished
Pallor:- absent
Icterus:- absent
Cyanosis:- absent
Clubbing:- absent
Generalized lymphadenopathy:- absent
Bilateral pedal edema :- absent
Vitals:-
Bp:120/80 mmhg
Pulse rate:-80 bpm
RR:- 18 cycles per min
Temp :-
Systemic examination:-
Abdomen:
On
inspection-
Shape of abdomen is elliptical and no scars. Umbilicus is inverted.
Normal movements and no visible pulsations.
On palpation-
On superficial palpation, abdomen is soft and non tender . No signs of ascites.
On deep palpation,
Liver: there is slight hepatomegaly
Sleep: there is slight splenomegaly
On percussion: tympanic note is heard
And no signs of ascites.
On auscultation:
Normal bowel sounds heard.
RESPIRATORY SYSTEM:
ON INSPECTION : position of trachea is central.
Slight drooping of right shoulder.
No intercoatal indrawing
No supraclavicular hallowness.
Shape and symmetry of chest -normal and symmetrical
No dilated viens and visible scars.
Accessory muscles of respiration -not prominent.
ON PALPATION:
on 3 finger test-trachea position central
Respiratory movements are decreased on right side
Measurement of left and right hemithorax-47cm equal on both sides
Ap diameter -23cm
Transverse diameter -31.5cm
Ap:transverse-5.75/7.87
Distance between vertebrae and infrascapular angle on right and left side is same=13.5cm
Vocal framitus :. Right. Left
Supraclavicular area. Reduced. N
Infraclavicular area. Reduced. N
Mammary area. Reduced. N
Axillary area Reduced. N
Infraxillary area Reduced. N
Suprascapular area. Reduced. N
Interscapular area. Reduced. N
Infrascapular area. Reduced. N
Percussion :
On direct percussion in clavicular area
On right side :
On left side :
Tidal percussion: dullness in the right 5 th intercostal space even after deep inspiration.
Traubes space percussion : dull note
Ascultation :
Vocal resonence :
Right left
Supraclavicular area. Reduced. N
Infraclavicular area. Reduced. N
Mammary area. Reduced. N
Axillary area Reduced. N
Infraxillary area Reduced. N
Suprascapular area. Reduced. N
Interscapular area. Reduced. N
Infrascapular area. Reduced. N
Decreased vesicular breath sounds on right side.
Bilateral air entry positive.
No crackles heard.
CVS Examination :
Inspection :
No abnormal palsations
No visible scars.
No chest deformities.
Mediastinum normal
Trachea central in position.
Palpation :
Mediastinal position : apex beat normal
Position of trachea central.
trachea central.
Percussion :
On percussion No cardiomegaly.
Ascultation : on examination of mitral area, pulmonary area, tricuspid area and aortic area S1 and S2 heard. No murmurs heard.
CNS : NAD
Investigations:-
USG:
ECG:
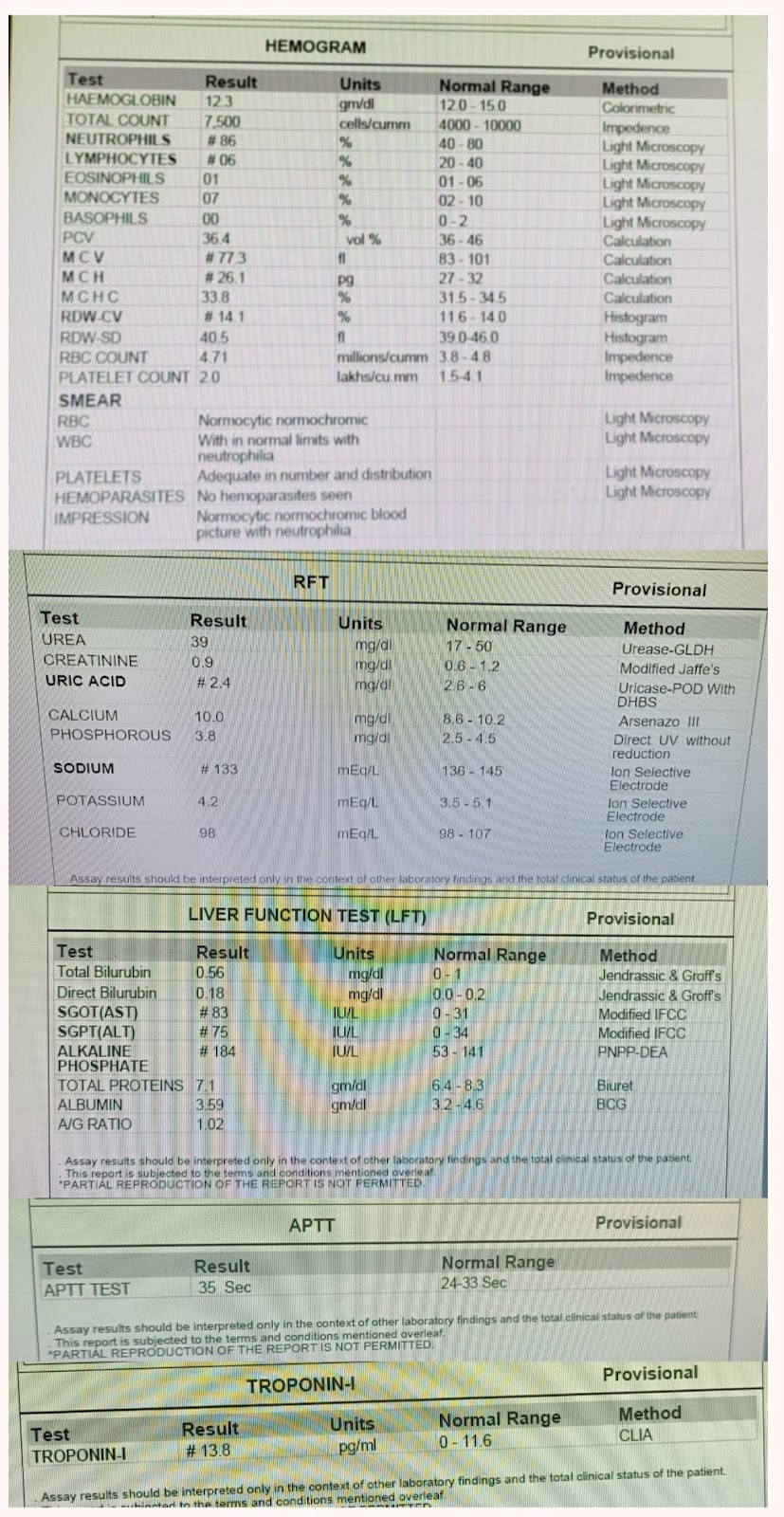
HEMOGRAM:
12/4/23
Provisional diagnosis:
pain abdomen under evaluation ?pleuritis
Dyselectrolytemia(resolve)
Bilateral mild pleural effusion (right>left).
Treatment:-
T.PAN 40MG PO/OD
T.PCM 650 MG PO/TID
INJ.NEOMOL 1MG IV/ SOS
IV FLUIDS NS @50ML/HR
T.MYORIL 4MG PO/SOS
INJ.TRAMADOL 1 AMP IN100 ML NS/TID
MONITOR VITALS.
SOAP notes
S
pain decreased
Fever spikes present
O
Patient is c/c/c
Temp:-100.6° F
PR- 82 bpm
RR-16 cpm
BP- 120/80mmHg
Spo2-100% at room Air
CVS- S1s2present, no murmurs heard
RS-B/L air entry present
N vesicular breath sounds
PA- soft,non tender
CNS - NFND
A
Pain abdomen under evaluation ? pleuritis
Dyselectrolytemia (resolved)
Right moderate Pleural effusion with underlying collapse and consolidation
Mild hepatosplenomegaly
P
IV FLUIDS NS @50ML/HR
INJ.NEOMOL 1GM IV /SOS IF TEMP >101 F
T.PCM 650 MG PO TID
INJ.TRAMADOL 1 AMP IN 100ML NS SOS
T.MYORIL 4MG PO/BD