21 year old female with anemia. July 04, 2023
21 year old female came to gm op with chief complaints of easy fatiguability ,light headedness since 7 years
C/o sob since 7 years ( sometimes )
No c/o Fever, burning micturation,vomitings, loose stools
No c/o involuntary movements or tingling sensation or numbness .
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 20 years back then she developed fever , edema over the fronto parietal region and irritability she was admitted in the hospital treated ( her hospital stay was around 10 days and she was discharged )
At the age of 3 years she had an episode of giddiness and was unconscious, she was again admitted in the hospital and then they were told that she had low levels of hemoglobin and she underwent blood transfusion.
At 15 years of age she was taken to the hospital for weakness, giddiness , she was admitted in the hospital and had second episode ofblood transfusion, her hemoglobin level improved to 9 after blood transfusion.
Few months after blood transfusion she started feeling weak and again went to the hospital , then her blood hemoglobin went down to 4 .
Since 3 to 4 months she complains of joint pains
Since 20 days she has allergy over her palms ,she has itching all over her hands relieved after taking medication at local hospital.
Since 20 days anasarca ( intermittently )
Resolved by its own . Last episode 2 days back
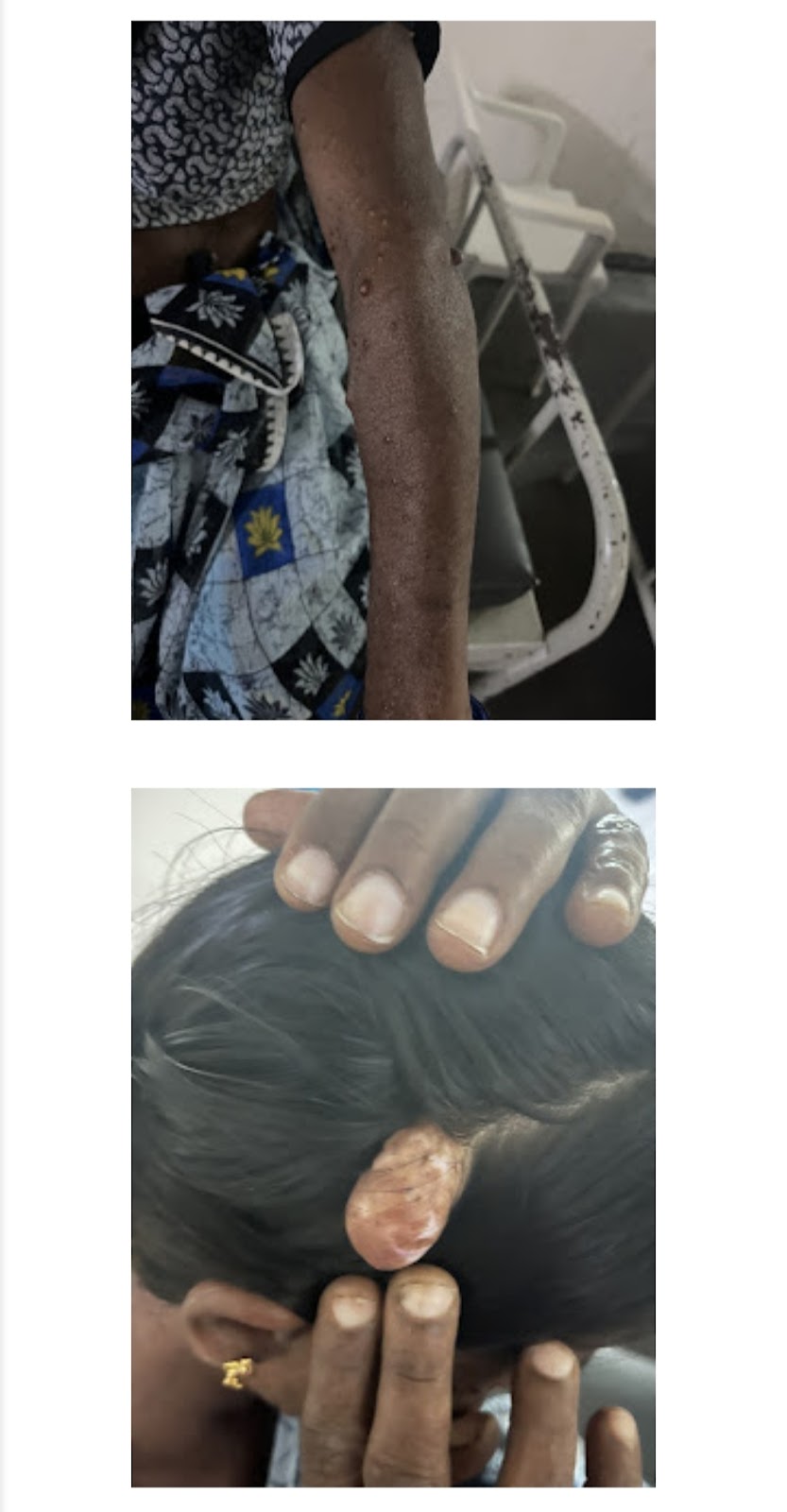
From 10 years of age she started noticing hyperpigmentation patches on her body which was slowly progressive to current stage .(neurofibromatosis )
Past history: history of trauma to head at the age of 10 while playing under a tree .
Daily routine:
Childhood
During the days she felt alright:
She wakes up at 6 Am ,does all the house hold work , she helps her mother and has breakfast at 8 Am and goes to school by walk (around 2 km ) , and comes back in the evening around 5 (by walk ) and plays with her friends and has dinner at 8 pm and goes to sleep by 10 pm
During summer holidays she went to work in the field ( cotton farms and chilli farms )
From morning 10 Am to evening 5 pm .
She studied till intermediate and didn’t go any further to college because of illness.
After progression of her illness she didn’t go to work in the fields , she helped her mother in all the household activities.
PAST History:
She is not a known case of DM, HTN, CVA, CAD, asthma, epilepsy.
FAMILY HISTORY:
Her sister has low value of hemoglobin (hb -6 gm/dl),but her sister doesn’t complain of any weakness.
Her mother has neurofibromatosis
GENERAL EXAMINATION:
Patient is conscious, coherent and co-operative.
Mooderately built and moderately nourished.
Pallor - present
Icterus - Absent
Cyanosis - Absent
Clubbing - Absent


No lymphadenopathy
Pedal edema- absent
Vitals :
Temperature - 98.2 F
Blood Pressure - 120/80mm hg
Pulse Rate - 82 bpm
Respiratory Rate - 16 cpm
SYSTEMIC EXAMINATION:
PER ABDOMINAL EXAMINATION:
INSPECTION-
Shape of abdomen : flat
Umbilicus : inverted
All quadrants of abdomen move with respiration
No visible peristalsis, pulsations, sinuses, engorged veins, hernial sites
PALPATION-
Abdomen soft
No local rise of temperature
No tenderness
Inspectors findings are confirmed
organomegaly - moderate splenomegaly
PERCUSSION:
Resonant note heard over all quadrants.
AUSCULTATION:
Bowel sounds heard
CVS EXAMINATION:
INSPECTION
The chest wall is bilaterally symmetrical
No dilated veins, scars or sinuses are seen
Apical impulse not visible
PALPATION:
Apex beat localised
AUSCULTATION:
S1 and S2 heard
No Murmurs
RS EXAMINATION:
INSPECTION:
Shape of chest: bilaterally symmetrical
Expansion of chest: Equal on both sides
Position of trachea: Central
No visible scars, sinuses, pulsations
PALPATION:
Inspectory findings confirmed
No tenderness, local rise of temperature
Normal expansion of chest on both sides in all areas
Position of trachea: Central
Vocal fremitus: resonant note felt
PERCUSSION:
Resonant note heard over all areas
AUSCULTATION:
BAE positive
Vocal resonance: resonant in all areas
CNS :No focal neurological deficit.
Provisional diagnosis:
Iron deficiency Anemia secondary to ? Blood loss ? Thalassemia minor k/c/o neurofibromatosis.
Investigations:
ECG
2d echo :
Trivial TR/AR/MR
No RWMA , NO AS/MS
Good LV systolic function, No diastolic dysfunction.
4/7/2023 investigations
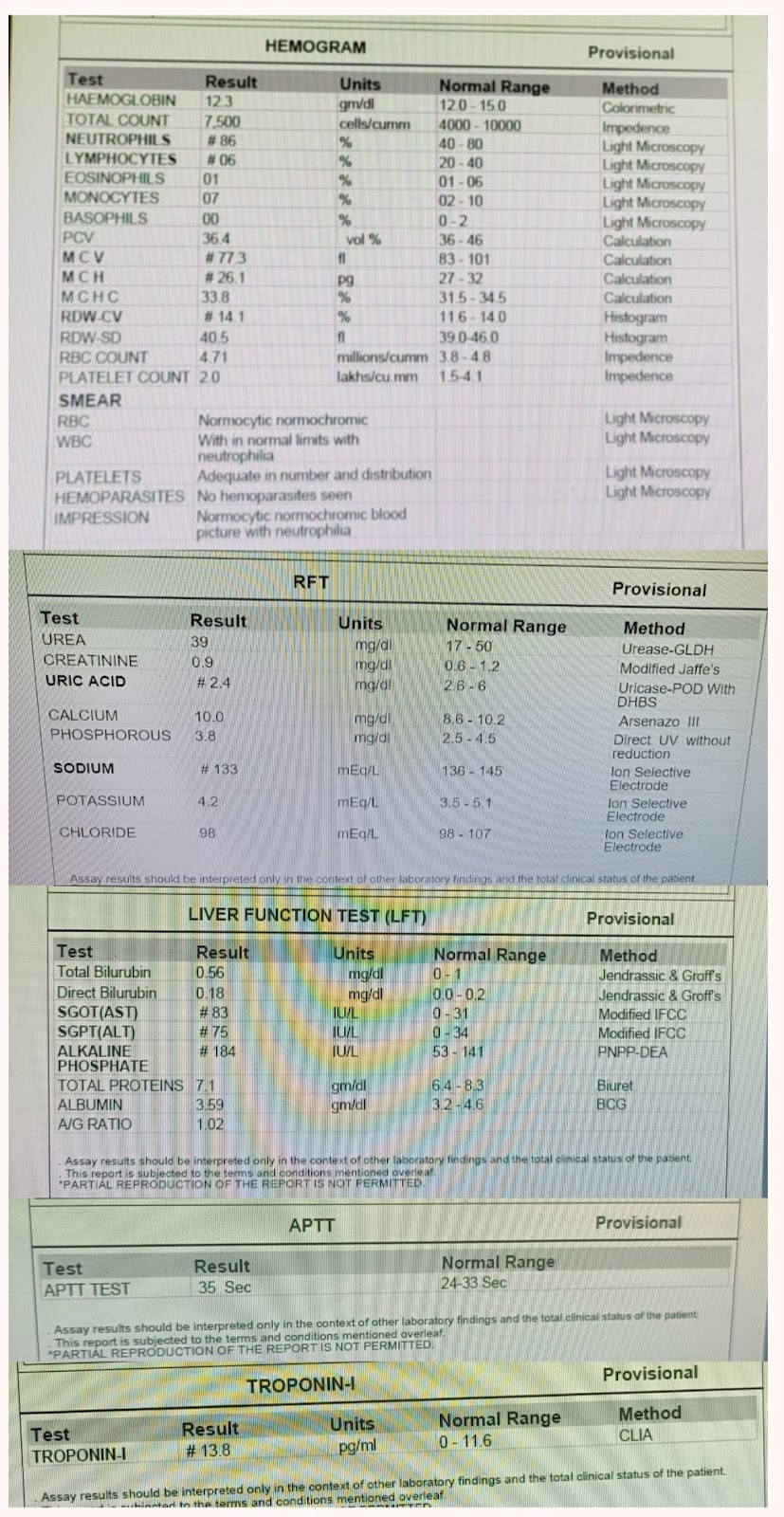
Hemogram :
Hb-6.4
TlC- 11200
N /L/E/M -35,19,41,5
PCV-25.9
MCV- 56.9
MCH-14.1
MCHC-24.7
RDW-27.2
Smear:
MICROCYTIC HYPOCHROMIC FEW PENCIL FORMS AND TARGET CELLS SEEN
WBC :normal limit with eosinophilia
Plt - adequate
BGT :A positive
RETICULOCYTE : 1.5
BLOOD UREA -18
SERUM CREATININE:0.6
Na - 140
K -4.7
Cl-102
LFT :
Total bilirubin: 0.49
Direct bilirubin:0.15
AST-14
ALT-10
ALP-128
TP:6.7
ALBUMIN: 4.35
A/g :1.85
Serology: negative.
Ultrasound 5/7/2023
Mild splenomegaly .
Serum ferritin :73.5 ng/ml
Stool for occult blood - negative
8-7-2023
HBA -98.4%
HBA2-1.6%
TIBC-394 ug/dl
TRANSFERRIN SATURATION -8%
UIBC-363.9ug/dl
IRON -30ug/dl
Hemogram 10. -7-23
Hb-6.8
TLC -7500
N -30 ,L-25 ,E-40 ,M-5 , B-0
PCV-27.3
MCV-59
MCHC -24.9
MCH-14.7
DISCHARGE SUMMARY:
Diagnosis:
IRON DEFICIENCY ANEMIA SECONDARY TO BLOOD LOSS ,NUTRITIONAL LOSS K/C/O NEUROFIBROMATOSIS
Case History and Clinical Findings :
C/O EASY FATIGUABILITY SINCE 7 YRS C/O SOB SINCE 7YRS
HOPI:
PT WAS APPARENTLY ASYMPTOMATIC 7 YRS AGO SINCE THEN HAS EASY FATIGUABILITY ,LIGHT HEADEDNESS , SOB GRADE 3 ,INSIDIOUS IN ONSET ,GRADUALLY PROGRESSIVE ,ORTHOPNEA PRESENT SOMETIMES C/O OCCASIONAL PALPITATIONS , C/O CONSTIPATION NO C/O FEVER ,BURNING MICTURITION ,VOMITINGS,LOOSE STOOLS NO C/O INVOLUNTARY MOVEMENTS,TINGLING SENSATION AND NUMBNESS H/O GENERALISED ITCHING 15 DAYS BACK H/O ANASARCA 15 DAYS BACK H/O BLOOD TRANSFUSION 3 YRS BACK AND WHEN SHE WAS 9 YRS OLD H/O NEUROFIBROMATOSIS NOT A K/C/O DM,HTN,SEIZURES,ASTHMA,TB
PERSONAL HISTORY
Diet
: MIXED APPETITE :
NORMAL BOWEL AND BLADDER
: REGULAR
ADDICTIONS : NONE SLEEP: ADEQUATE
GENERAL EXAMINATION PATIENT IS CONSCIOUS /COHERENT/CO OPERATIVE PALLOR PRESENT NO ICTERUS,CYANOSIS,CLUBBING,LYMPHADENOPATHY,OEDEMA VITALS TEMP : AFEBRILE PR : 84 BPM RR: 18 CPM BP : 140/90 MMHG
SYSTEMIC EXAMINATION
CVS : S1,S2 HEARD ,NO MURMURS
RS: BLAE PRESENT
P/A : SOFT,NON TENDER
CNS: NO FOCAL NEUROLOGICAL DEFICITS
OPHTHALMOLOGY REFERRAL ON 6/7/23 RIGHT EYE : REFRACTION - 4.50 SPH ,0.50 CYL X40* -6/9 IRIS SHOWS LISCH NODULES LEFT EYE : REFRACTION - 4.50 SPH ,0.50 CYL X 60 * - 6/9 ,LIDS - UL PUS POINT PRESENT IRIS SHOWS LISCH NODULES FUNDUS STUDY IS NORMAL ADVICE USE SPECTACLES FOR REFRACTION ERROR
Investigation 2D ECHO WAS DONE ON 4/7/23 WHICH SHOWED EF : 62% ; IVC 0.6 COLLAPSING ; RVSP : 36 mmHg TRIVIAL TR/MR/AR NO RWMA, NO AS/MS GOOD LV SYSTOLIC FUNCTION
NO DIASTOLIC DYSFUNCTION ,NO PAH/PE USG DONE ON 5/7 MILD SPLENOMEGALY 13 CM INCREASE SIZE ON 4/7
BLOOD GROUP : A POSITIVE RETICULOCYTE COUNT : 1.5 % HEMOGRAM HB: 6.4 GM/DL TLC : 11,200 CELLS /CUMM N/L/E/M/B : 35//19/41/05/00 PCV : 25.9 VOL% RBC COUNT : 4.55 MILLIONS/CUMM PLATELET COUNT : 4.26 LAKHS/CUMM PERIPHERAL SMEAR : RBS SHOWS MICROCYTIC HYPOCHROMIC WITH FEW PENCIL FORMS AND TARGET CELLS WBC SHOWS WITHIN NORMAL LIMITS WITH EOSINOPHILIA PLATELET ADEQUATE LFT T.B : 0.49MG/DL D.B : 0.15 MG/DL SGOT: 14 IU/L SGPT: 10 IU/L ALP :128 IU/L T.P: 6.7 GM/DL ALBUMIN :4.35 GM/DL A/G RATIO : 1.85 HBS AG RAPID : NEGATIVE ANTI HCV ANTIBODIES RAPID : NEGATIVE
SERUM CREATININE : 0.6 MG/DL SERUM ELECTROLYTES : SODIUM/POTASSIUM / CHLORIDE/CALCIUM IONIZED : 140/4.7/102/1.06 BLOOD UREA : 18 MG/DL CUE ALBUMIN ,SUGARS NIL PUS CELLS ; 2 TO 3 STOOL FOR OCCULT BLOOD : NEGATIVE FERRITIN : 73.5 NG/ML ON 6/7 PERIPHERAL SMEAR RBC : ANISOPOIKILOCYTOSIS WITH HYPOCHROMASIA PREDOMINANTLY MICROCYTES FEW TEAR DROP CELLS INCREASED IN COUNT WITH EOSINOPHILIA PLATELET ADEQUATE IMP- MICROCYTIC HYPOCHROMIC ANEMIA WITH EOSINOPHILIA ON 8/7 HEMOGLOBIN ELECTROPHORESIS Hb A : 98.4% Hb A2 : 1.6 % IRON STUDIES TIBC : 394 UG/DL TRANSFERRIN SAT : 8% UIBC : 363.99 UG/DL PHOTOMETRY : 30 UG/DL
Treatment Given(Enter only Generic Name) 1.INJ IRON SUCROSE 200MG IN 100ML NS IV/OD OVER 30 TO 40 MIN GIVEN ON 4/7 ,5/7 , 7/7 ,9/7/23 2.TAB .OROFER XT PO/OD
Advice at Discharge
1.TAB.OROFER XT PO/OD [X-1-X] FOR 30 DAYS
2.TAB.LIMCEE PO/OD [X-1-X] FOR 30 DAYS 3.TAB.MVT PO/BD [X-1-1] FOR 30 DAYS 4.IRON RICH DIET